



CoQ10 and Statins — What UK Patients Need to Know
-
By Chris Jones
Written by Chris Jones, Social Media Manager at Nutrivity with 7+ years in the supplement industry.
CoQ10 and Statins — What UK Patients Need to Know
Statins are the most prescribed class of medication in the UK, taken by an estimated 8 million people for the prevention and treatment of cardiovascular disease. They are effective at lowering LDL cholesterol and reducing cardiovascular events — and they have a well-documented side effect that most patients are never told about: they deplete CoQ10. The mechanism is biochemical, the evidence is well-established, and the clinical consequences — particularly muscle pain and fatigue — affect a significant proportion of statin users.
This guide explains how statins deplete CoQ10, what the clinical consequences are, what the research on CoQ10 supplementation in statin users shows, and what UK patients taking statins need to know before deciding whether to supplement. For full information on Nutrivity’s high-strength CoQ10, visit our CoQ10 300mg Vegan Capsules product page.
How Statins Deplete CoQ10
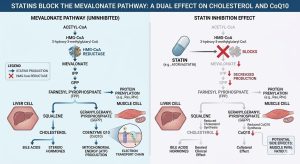
To understand why statins deplete CoQ10, you need to understand the mevalonate pathway — the biochemical route the body uses to produce both cholesterol and CoQ10.
The mevalonate pathway is a sequence of enzymatic reactions that begins with acetyl-CoA and produces a range of biologically important compounds. Cholesterol is one end product. CoQ10 is another — it branches off the same pathway at a later stage. Statins work by inhibiting HMG-CoA reductase, the enzyme that controls the early rate-limiting step of this pathway. By blocking this step, statins reduce the production of all downstream products — including CoQ10.
This is not a side effect of statin contamination or a manufacturing issue. It is a direct and unavoidable biochemical consequence of how statins work. Every statin, regardless of type or brand, inhibits the same pathway and therefore reduces CoQ10 synthesis to some degree. The extent of depletion varies between statins and between individuals, but the mechanism is the same.
Multiple studies have measured plasma and tissue CoQ10 levels in statin users and found consistent reductions of 30–50% compared to non-users. For a compound that is already declining with age in most statin-taking adults, this pharmacological depletion represents a significant additional reduction on top of the age-related baseline.
Clinical Consequences — Muscle Pain, Fatigue, and More
The most clinically significant consequence of statin-induced CoQ10 depletion is its impact on muscle tissue. CoQ10 is essential for mitochondrial energy production in muscle cells. When CoQ10 levels fall, the capacity of muscle mitochondria to generate ATP is reduced — and this manifests as muscle symptoms in susceptible individuals.
Statin-associated muscle symptoms (SAMS) affect an estimated 10–15% of statin users in clinical practice, though some observational studies suggest the real-world figure may be higher. Symptoms range from mild muscle aches and cramps to significant weakness and, in rare cases, the serious condition rhabdomyolysis — the breakdown of muscle tissue that can cause kidney damage. In the majority of affected patients, symptoms are mild to moderate and resolve on stopping the statin, but they are a significant cause of statin discontinuation — which in patients with established cardiovascular disease carries real clinical risk.
Beyond muscle symptoms, statin-induced CoQ10 depletion may contribute to the fatigue reported by some statin users, given CoQ10’s role in systemic energy production. Some research also suggests a potential contribution to cognitive effects reported with certain statins, though this area is less well-established.
What the Research Shows on CoQ10 Supplementation in Statin Users
The research on CoQ10 supplementation for statin-associated muscle symptoms has produced mixed results, which is worth understanding in context.
Several well-designed RCTs have shown significant reductions in muscle pain intensity in statin users taking CoQ10 compared to placebo. A 2014 study published in the Medical Science Monitor found that CoQ10 at 100mg twice daily significantly reduced statin-associated muscle pain and its interference with daily activities. Other studies have shown improvements in exercise tolerance and reductions in fatigue scores.
However, other trials have found no significant benefit, and systematic reviews have produced inconclusive overall conclusions. This variability in results may reflect differences in the dose of CoQ10 used (many studies have used lower doses of 100–200mg, whereas the theoretical rationale supports higher doses), differences in which statin patients received, differences in baseline CoQ10 levels, and differences in how muscle symptoms were measured and reported.
The important clinical context is this: CoQ10 supplementation has an excellent safety profile, is well tolerated, and has a clear mechanistic rationale in statin users. Where the evidence is mixed on muscle symptoms, the cost-benefit calculation for most statin users is straightforward — the potential benefit is meaningful, the risk is negligible, and many cardiologists recommend it routinely for patients experiencing muscle symptoms.
What UK Statin Patients Should Know
Your GP may not have mentioned CoQ10. Despite the well-established mechanistic link between statins and CoQ10 depletion, routine CoQ10 supplementation is not part of standard NHS prescribing guidance for statin users. Many GPs are aware of the connection but will not proactively recommend CoQ10 unless asked, in part because the RCT evidence on muscle symptoms is mixed and in part because it falls outside standard prescribing pathways. This does not mean it is not worth considering — it means the decision rests with the patient.
If you are experiencing muscle pain or fatigue on statins, CoQ10 is a reasonable first step. Before requesting a statin change or considering stopping your medication — both of which carry cardiovascular risk in patients on statins for established disease — a trial of CoQ10 supplementation is a low-risk, low-cost intervention worth trying. Always discuss changes to your statin regimen with your GP.
Dose matters. Many UK CoQ10 supplements provide 30–100mg — below the doses used in most of the positive research in statin users. At Nutrivity, we provide 300mg per capsule, which is at the higher end of the therapeutic range used in clinical studies and is the dose most likely to meaningfully restore depleted CoQ10 levels.
CoQ10 does not reduce the cholesterol-lowering efficacy of statins. There is no evidence that CoQ10 interferes with the primary mechanism of statin action. Taking CoQ10 alongside a statin does not reduce the cardiovascular benefit of the medication. Read our full article on What is CoQ10 benefits and dosage guide.
Which Statin Depletes CoQ10 the Most?
All statins deplete CoQ10 through the same mevalonate pathway mechanism. However, the degree of depletion varies with the potency and lipophilicity (fat-solubility) of the statin. More potent statins — particularly atorvastatin and rosuvastatin, which are the most widely prescribed in the UK — tend to produce greater CoQ10 depletion than older, less potent statins such as pravastatin and fluvastatin. Lipophilic statins (atorvastatin, simvastatin, lovastatin) also penetrate muscle tissue more readily, which may contribute to their higher rate of muscle symptoms compared to hydrophilic statins.
If you are taking atorvastatin or rosuvastatin — the two most commonly prescribed statins in the UK — and experiencing muscle symptoms or fatigue, CoQ10 supplementation is particularly worth considering.

Summary — CoQ10 for Statin Users in the UK
The link between statin use and CoQ10 depletion is well-established biochemically and clinically. For the estimated 8 million statin users in the UK, many of whom experience muscle symptoms or fatigue, CoQ10 supplementation represents a low-risk, mechanistically sound intervention that many cardiologists recommend as a first step before altering the statin regimen. The key variable is dose — 300mg daily is at the level used in the research showing the most consistent positive results, and is substantially higher than most products available in the UK market.
For full product information, visit Nutrivity’s CoQ10 300mg Vegan Capsules product page.
Frequently Asked Questions
Do statins deplete CoQ10?
Yes. Statins inhibit the HMG-CoA reductase enzyme, which is part of the mevalonate pathway used to produce both cholesterol and CoQ10. By blocking this pathway, statins reduce CoQ10 synthesis as an unavoidable biochemical consequence. Studies have measured plasma CoQ10 reductions of 30–50% in statin users compared to non-users.
Should I take CoQ10 with statins?
If you are experiencing muscle pain, weakness, or fatigue on statins, CoQ10 supplementation is a reasonable and low-risk intervention to try. The mechanistic rationale is clear, the safety profile is excellent, and several clinical studies have shown benefit for muscle symptoms. Discuss with your GP before making any changes to your statin regimen.
What dose of CoQ10 should statin users take?
Clinical studies in statin users have used doses ranging from 100mg to 300mg daily. At Nutrivity, we provide 300mg per capsule — at the higher end of the therapeutic range used in research and more likely to meaningfully restore depleted CoQ10 levels than the 30–100mg products common in the UK market.
Does CoQ10 interfere with statins?
No. There is no evidence that CoQ10 reduces the cholesterol-lowering efficacy of statins or interferes with their cardiovascular protective mechanism. CoQ10 and statins can be taken together safely. As always, inform your GP of any supplements you take alongside prescription medication.
How long before CoQ10 helps statin muscle pain?
Most studies showing benefit for statin-associated muscle symptoms have run for 30–90 days. A reasonable trial period is 8–12 weeks of consistent supplementation at an adequate dose before assessing whether symptoms have improved.
Is Nutrivity's CoQ10 suitable for statin users?
Yes. Nutrivity’s CoQ10 300mg provides the higher end of the therapeutic dose used in clinical research, in HPMC vegetable capsules with no unnecessary additives. Full ingredients are published on the product page. Always consult your GP before making changes to your supplement or medication routine.